Repetitive transcranial magnetic stimulation (rTMS) is an established clinical intervention, but its effectiveness depends on precision and reproducibility.
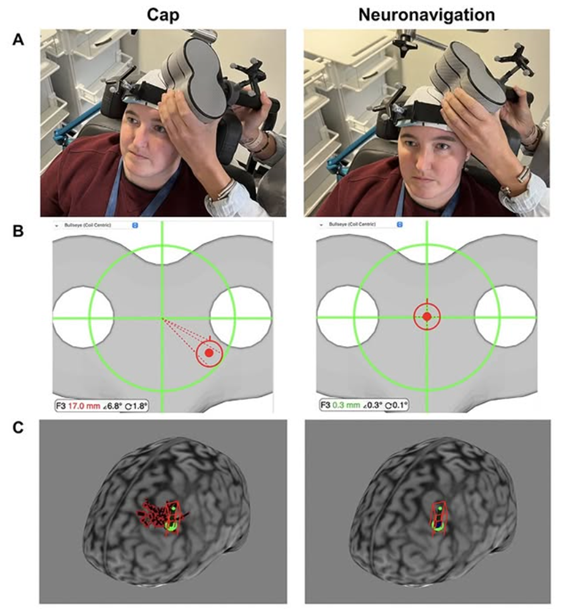
Neuronavigation represents a significant advance over traditional scalp-based targeting methods. By using each patient’s structural MRI, neuronavigation enables anatomically accurate targeting. This approach accounts for interindividual variability in skull anatomy, cortical folding, and brain–scalp distance. As a result, stimulation is delivered to the intended cortical region rather than an approximate scalp location.
Neuronavigation also improves session-to-session reproducibility. In repetitive protocols, consistent coil placement across days or weeks is critical for therapeutic efficacy. Millimetric accuracy ensures reliable engagement of the same neural substrate over time. Another key advantage is the reduction of operator-dependent variability. Landmark- or cap-based methods are sensitive to clinician experience and positioning errors. Neuronavigation standardizes targeting across operators and clinical settings. In addition, precise control of coil orientation relative to cortical gyri optimizes the induced electric field. This increases physiological specificity and may enhance clinical outcomes.
Finally, neuronavigation improves safety, documentation, and quality control. Real-time feedback and detailed logs support traceability and facilitate the integration of clinical care with research-driven protocols.
TMS Buran team